
When epidemiologist Maeve Wallace first began publishing national data on pregnancy-associated homicide and suicide nine years ago, she knew that more granular numbers would be essential to implementing effective prevention. Her findings set her on a path toward addressing incomplete state-level data, and nearly a decade later, she and her team are finally on equal footing with nationwide research. In February, they published a landmark study calculating pregnancy-associated violence by state, and the report suggests a strong connection to firearm legislation and reproductive protocols.
“I think the vast variation that we see across states in terms of their health outcomes, especially maternal mortality or pregnancy-associated death, speaks to the difference in policy,” said Wallace, a perinatal epidemiologist at the University of Arizona.
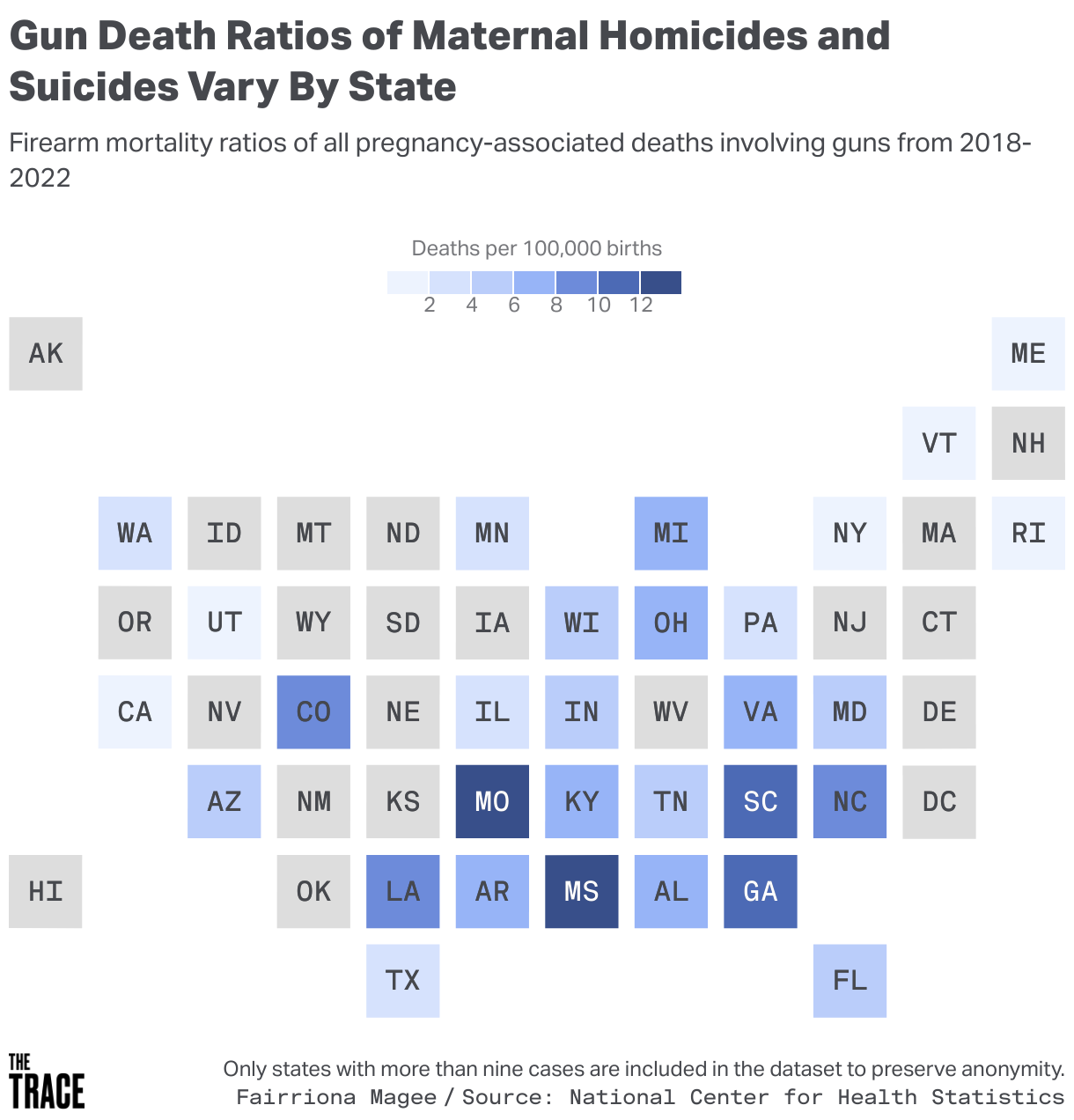
The study, published in the Journal of the American Medical Association, is the first to use nationally available data to calculate state-specific rates of pregnancy-associated violence, or violence during pregnancy and up to one year postpartum. The researchers analyzed violent and substance-related pregnancy deaths between 2018 to 2022 and found that 76 percent of pregnancy-associated homicides were attributed to firearms, while 37 percent of suicides involved a firearm. Mississippi, which has one of the highest rates of obstetric-related complications in the country, had the highest maternal death ratio by firearm in the United States, with 13.42 deaths per 100,000 births.
“If it were entirely due to biological factors, we wouldn’t see any state-level differences, so we know for sure, it’s something beyond biology,” said Jaquelyn Jahn, a social epidemiologist at Drexel University and an author of the study. “How can the maternal care environment differ so much; how do the policy environments differ; how do the histories differ, which could all potentially affect whether pregnant people in those states live or die.”

For decades, epidemiologists have known that homicide is a leading cause of death for pregnant women and birthing people in the United States, surpassing obstetric-related causes including sepsis or hemorrhaging. As the nation’s homicide numbers peaked in the 1980s, retrospective research began to uncover an uptick in pregnancy-related violence, mostly attributed to firearms. But, as The Trace reported last year, it wasn’t until 2003 that the Centers for Disease Control and Prevention began marking pregnancy status on death certificates, and it would take nearly 15 years before the health agency had data from each state.
After Mississippi, the study showed Missouri, Georgia, South Carolina, Colorado, Louisiana, and North Carolina all had the highest ratios of pregnancy-associated firearm violence. Of those six states, all had some form of permitted open-carry laws. Each state, besides Colorado, also had some form of an abortion ban at the time the data was collected, with Mississippi and Louisiana being the most restrictive. Multiple studies have found that states with more restrictive reproductive policies have higher rates of pregnancy-associated violence and an increased likelihood of interpersonal violence among pregnant patients.
“One really striking thing from this analysis is that it just shows the extent of firearms and the role of firearms in pregnancy-associated homicides,” Jahn said. “It’s really an alarming number of cases regarding homicide, but [firearms] are also a strong contributor to pregnancy-associated suicides.”
Like several of the other states with the highest pregnancy-related homicide rates, Mississippi has one of the highest firearm mortality rates in the country. The state does not require background checks for open carry, lacks extreme risk protection orders and domestic violence gun laws, and does not prohibit assault weapons. Conversely, of all the top six states with the highest rates of maternal firearm violence, Mississippi has the most restrictive reproductive laws in the country. The state completely banned abortion outside of life-saving care following the Supreme Court’s 2022 Dobbs decision and has not expanded Medicaid to include state funds to cover abortion for Medicaid beneficiaries.
Though the authors acknowledge their study is descriptive, laying out the scope of the problem without specifically comparing state-by-state policies, they said future research is imperative.
Jahn underscored that these estimates are an undercount, and for so many violent deaths among women, pregnancy status is unknown. “The rates that we were able to estimate are from people who died and for whom we know their pregnancy status, and that is a big caveat to understanding the findings. [It’s] an area where we need a much more robust public health monitoring system to be able to have better data on these factors.”
The study separately calculated the averages for firearm suicide and homicide and found that firearms accounted for as many as 15 percent of pregnancy-associated deaths in Colorado. Colorado has relatively strict gun laws compared to other states with high rates of violent death among pregnant people and also relatively progressive reproductive laws. But the state had the highest ratio of pregnancy-associated firearm suicide at 5.45 deaths per 100,000 births, followed by Missouri, Georgia, and Virginia. Although Colorado had the highest firearm suicide ratio, pregnancy-associated mortality was highest in Montana, with 21.55 deaths per 100,000 live births.
Research has found that pregnancy-related suicide victims tend to be older white or Native American women. This differs from pregnancy-associated firearm homicide, which disproportionately affects young Black women. Wallace, Jahn, and other epidemiologists note that addressing both lies in continued funding of public health monitoring and infrastructure, and state policy initiatives to enhance interpersonal violence screening and postpartum support.
“Every death, every number that you see in these types of publications could have been prevented,” Wallace said. “This is not an inevitable situation and we have to underscore that there are ways that we can prevent this.”
Correction: A previous version of this story stated that Mississippi, not Missouri, had the second-highest ratio of pregnancy-associated firearm suicide. This story has been updated.
